P. Maló1, C. Vidal2, C. Almeida2, I. Festas2, J. Nunes2, M. De Araújo Nobre3 1DDS, PhD, Oral Surgery Department; Maló Clinic Lisbon, Portugal 2DDS, Prosthodontic Department; Maló Clinic Lisbon, Portugal 3RDH, MSc Epi, Research and Development Department; Maló Clinic Lisbon, Portugal
The rehabilitation of total edentulous patients is associated to several limitations (decay, overloading of remaining teeth, Periodontitis etc.). The implant-supported solutions represent an alternative to restore masticatory function, phonetics and aesthetics, increasing the comfort and the patient self esteem, only possible with a fixed rehabilitation1-3. Implant-supported rehabilitation of posterior maxillary areas with high bone resorption is a challenge to Dentistry due to anatomical limitations, such as the presence of noble structures (maxillary sinus and the inferior dental nerve) and the low bone density associated to high functional load supported by this area4-7. Different procedures have been presented to rehabilitate maxillary posterior areas with reduced height and width. A less invasive procedure could involve the insertion of short implants. However, when in the presence of an atrophic jaw limiting the area even for the insertion of a short implant, one could consider other techniques such as angulated implants7-9. The All-on-4 Concept (Nobel Biocare AB, Gothenburg, Sweden) presents as a surgical option in this type of rehabilitation, associated with numerous advantages such as: simplified and functional rehabilitation of a maxillary with only 4 implants; high primary stability of all implants allowing immediate function; reduction of prosthetic cantilevers; avoiding bone grafting; and a high success rate4-5. The development of the concept led to the application in the rehabilitation of complete edentulous atrophic maxillae using an extra-maxxilary approach for inserting zigomatic implants either alone (4 zygomatic implants – All-on-4 Double Zygoma) or in combination with standard implants (All-on-4 Hybrid)6.
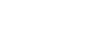
1. Pre-operative orthopantomography.
The flexibility of the All-on-4 principle was tested in a clinical study by applying it to the posterior partial rehabilitation of atrophic jaws: by inserting 2 implants (anterior implant placed in axial position, posterior implant tilted distally) supporting a 3 to 4 unit bridge, a 98.8% implant survival rate and low marginal bone resorption were registered in the long-term follow-up10. The concept design in this particular area was aimed at avoiding several factors such as a straight implant alignment, suboptimal implant size, or the use of cantilevers in order to decrease the potential bending forces of the implants. For the definitive prosthetic rehabilitation of the upper jaw of total edentulous patients, the rehabilitation with the MaloClinic Ceramic Bridge emerges as the ideal treatment option: This prosthetic rehabilitation solution is fabricated with individual Procera crowns (Zirconia copings and Nobel Rondo Zirconia Ceramic; Nobel Biocare AB) cemented onto a CAD/CAM fabricated Ti framework (Nobel Biocare AB) with pink acrylic resin (PallaXpress Ultra, Heraeus Kulzer GmbH) that replicated the missing gingival tissues11. This innovation, apart from providing high aesthetics and biocompatibility, facilitates the repairing of any crown.11 The use of screwed solutions presents advantages related to access, retrievability and management of the peri-implant soft tissues in the rehabilitation of small bridges and unitary crowns over implants12. The aim of this case report is to illustrate the rehabilitation of atrophic jaws using the All-on-4 Concept (Nobel Biocare AB) applied to the partial and complete edentulous rehabilitations of atrophic jaws in a multidisciplinary environment.
2. Extra-oral pre-operative view.
3. Intra-oral pre-operative view.
Case description
Pubblicità
Female patient, aged 65, attended the private practice (Maló Clinic Lisbon, Portugal) complaining about her present rehabilitation with removable prostheses associated with diminished masticatory capability and esthetic appearance. Her main goal was to obtain
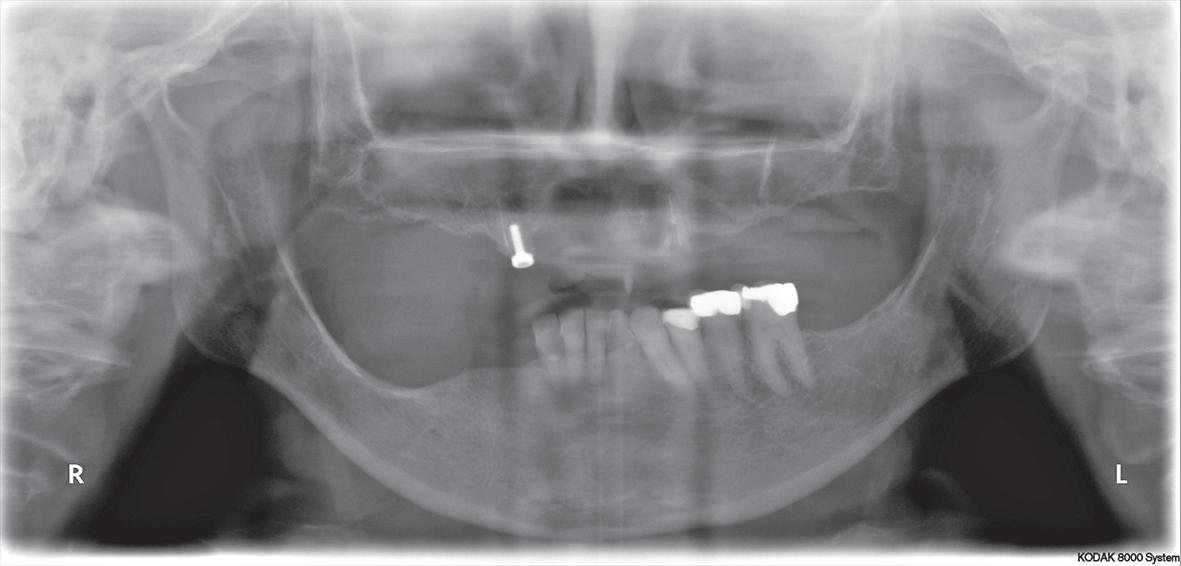
4. Post-operative orthopantomography. Maxillary rehabilitation through the All-on-4 Hybrid and Mandibular rehabilitation through the Partial All-on-4 principle.
an upper and lower implant-supported fixed rehabilitation. After careful clinical and radiographic examination it was proposed to rehabilitate the upper and lower jaws according to the All-on-4 Concept (Figures 1-3). In the same surgical procedure, 2 zygomatic implants with 40 mm and 45 mm length (Nobel Biocare AB) were inserted in the posterior region and 2 standard maxillary implants (NobelSpeedy Groovy 4×13 mm RP, Nobel Biocare AB) were inserted in the anterior region of the maxilla, following the All-on-4 Hybrid (Nobel Biocare AB) protocol6. All implants achieved an insertion torque above 50N/cm which allowed immediate provisionalization (Figures 4-6). In the lower jaw, 2 implants were placed on the 4th quadrant, one distally tilted implant (NobelSpeedy Groovy RP 4x13mm, Nobel Biocare) and one axial implant (NobelSpeedy Groovy NP 3,3x13mm, Nobel Biocare)10 followed by their respective rehabilitation with screw-retained acrylic provisional crowns replacing crowns #43 to #46 (Figures 5, 6). In order to correct the occlusal plan and considering the previous extensive fillings, endodontic treatments, reinforced glass fiber posts (D.T. Light-Post Bisco Inc.; Schaumburg, USA) and provisional crowns (Heraeus Kulzer Premium Linie, Heraeus Kulzer GmbH&Co., Wasserbutg, Germany) were performed in the teeth #34 to #36. A maintenance protocol with post-operative after 2, 4 and 6 months were performed, and in the absence of signs or symptoms of peri-implant pathology, the final rehabilitation was scheduled. Taking into consideration the age, the biomechanical advantages and the patient’s aesthetic concerns, a MaloClinic Ceramic Bridge (individual Procera crowns, Zirconia copings and Nobel Rondo Zirconia Ceramic; Nobel Biocare AB) cemented onto a CAD/CAM fabricated Titanium framework (Nobel Biocare AB) with pink acrylic resin (PallaXpress Ultra, Heraeus Kulzer GmbH) was performed in the maxilla. In the mandible, a screw-retained metal-ceramic fixed partial denture was performed over the 4th quadrant implants replacing crowns #43 to #46, and individual metal-ceramic crowns were luted with GC Fuji Plus (GC, América, Inc.) to the abutments #34 to #36 (Figures 7-12). The patient was kept on a six month recall plan, and both rehabilitations remained stable through a complete follow-up period of 3 years.
5. Extra-oral view of the immediate prosthesis.6. Intra-oral view of the immediate prosthesis.
Rehabilitation of atrophic jaws using the All-on-4 Concept
- Ultima modifica: 2013-03-15T15:26:03+00:00
da Redazione









{kind=link}